
reviews


Premature ejaculation is often a punchline.
However, for the estimated one in three men who will cope with premature ejaculation at some point in their lives, the laughs only go so far.
When the lights go out in the bedroom, premature ejaculation is no laughing matter.
Sex is a basic human need — not just our own gratification, but the need to feel sexy and valuable to a partner who finds the experience equally gratifying.
Most men who suffer from premature ejaculation go through the emotional wringer. They feel inadequate as lovers, as partners, as men.
When they most want to satisfy their romantic partners, they often fall short.
It's time to get serious about the toll premature ejaculation takes on the men who experience it. It's time to work compassionately toward a solution.

If you suffer from premature ejaculation, you are not alone.
Many men have weathered this condition, and gone on to have satisfying sex lives, marriages, children.
This guide breaks down premature ejaculation to the nitty-gritty, including:
On a basic level, premature ejaculation is when a man ejaculates sooner than he would like to.
Premature ejaculation does have a technical definition.
The International Society for Sexual Medicine (ISSM) defines it as,
“Ejaculation that always or nearly always occurs prior to or within about 1 minute of vaginal penetration from the first sexual experience (lifelong PE)
or a clinically significant and bothersome reduction in latency time, often to about 3 minutes or less (acquired PE).”
There are two main types of premature ejaculation:
Premature ejaculation may be caused by:
If you are experiencing only occasional early ejaculation, this may not be a cause for concern.
However, more frequent premature ejaculation is likely to cause distress in a relationship, leaving both partners unsatisfied.

The symptoms of premature ejaculation are:
Notice that feelings of distress over the condition is a key symptom.
If ejaculating quickly doesn’t cause distress or anxiety, there is no real condition or pathology.
The first step in fixing a problem is acknowledging that you have a problem.
So how can you diagnose PE?
If a sexually active man knows that he cannot control his ejaculatory response, and feels embarrassed or inadequate over the condition, that is typically plenty.
No further testing is needed.
A conversation with your doctor, if you feel it is necessary, is also usually enough to facilitate a diagnosis of premature ejaculation.
There are no monitors or machines that diagnose premature ejaculation and your Physician will rely solely from your firsthand account of sexual activity.
To diagnose premature ejaculation, doctors look for an IELT time of two to three minutes or less.
IELT is short for "intravaginal ejaculatory latency time." It refers to the time (in minutes, seconds, hours, etc.) between vaginal penetration and ejaculation.

Some men feel too ashamed of sexual dysfunctions to bring them up, even with their doctors.
This is unnecessary. Sex is a bodily function, critical to achieving a high quality of life for most human beings.
Every doctor worth his or her medical license acknowledges the importance of sex, and takes sexual satisfaction very seriously.
Below is a list of questions to try to self-diagnose premature ejaculation and get a better understanding of what category of PE you may fall into.
If you answer ‘yes’ to any or all of the questions under a sub-type of premature ejaculation you are at a good starting point to resolve and understand your symptoms better.
The male arousal and ejaculatory cycle is complex.
Many different hormones, neuropathways, and organs contribute to male arousal, orgasm, and ejaculation.
The testicles play starring roles by producing testosterone. This hormone stimulates sexual desire (libido).
Many factors contribute to libido, and a study done by a team of Urologists including Dr. Mohit Khera showed that increasing testosterone levels in men lead to higher libido.
Note; Women naturally produce testosterone as well, and there too it contributes to sexual arousal.
Male arousal has six distinct stages:
When a man is stimulated visually, physically, or emotionally in a sexual manner, the brain releases the neurotransmitter acetylcholine.
This neurotransmitter causes nitric oxide to dilate which results in increased blood flow into the penis, causing blood to flood into them and produce an erection.
This response is usually accompanied by rapid respiration, retraction of the scrotum, and increased tension in the muscles.
As physical sexual stimulation of the penis increases, the man's urge to thrust his pelvis becomes involuntary. The heart rate, blood pressure, and body temperature all increase.
Seminal fluid (pre-cum) leaks into the urethra to balance its internal pH, increasing the chance that sperm cells will survive the ensuing passage.
Sometimes referred to as the "point of no return."
The body produces semen by mixing sperm from the testicles with seminal fluid from the prostate. They mix in the seminal vesicle.
Ejaculation is now imminent.
Involuntary spasms throughout the pelvis force the semen out of the seminal vesicle, through the urethra, and out of the tip of the penis.
The reward center of the brain gets showered with neurochemicals, triggering an intense euphoric response.
Meanwhile, the lateral orbitofrontal cortex behind the left eye, where judgment and self-control live, actually shuts down, creating a sense of indifference to anything other than the orgasm.
The penis begins to lose its erection. The bath of chemicals the brain just received causes extreme relaxation and drowsiness.
During the refractory period, the man is physically unable to achieve another erection. Younger men may experience shorter refractory periods than older men.
No one root cause can explain every case of premature ejaculation.
The diagnosis describes the condition, not the source of the condition. A persistent premature ejaculation problem can usually be traced to one or more of the following issues:
A man's early sexual experiences may set a pattern for future sexual experience.
There are many ways in which first forays into sexuality can imprint him with a propensity for premature ejaculation.
An inexperienced man may become so aroused by his first sexual experiences that he is overwhelmed by sensation.
Lacking the practice with ejaculatory control, he may not be able to delay the orgasmic response.
He may be able to detect his partner's disappointment at the short duration of the sexual encounter and develop anxiety over his ability as a lover.
This anxiety may translate into future trouble with ejaculatory control.
The source of the problem may also predate the man's first experiences with a partner.
Note; A young man's very first sexual experiences are often masturbation.
If the man is young enough—say, a preteen or teenager—he probably lives with parents, siblings, and other family members.
Privacy may be at a minimum, the threat of disapproval or mockery very real.
A young man in this situation may learn to achieve orgasm through masturbation as quickly and discreetly as possible.
This habit of fast ejaculation can persist into experiences with a partner.
Familial disapproval of sex may also prompt a man to rush to orgasm during sex with a partner.
A man who has experienced erectile dysfunction in his early sexual experiences, paradoxically, may also develop premature ejaculation.
A study from the Translational Andrology and Urology showed that some men may be concerned that their erection won't last, so he gets into the habit of rushing to climax before losing it.
Poor body image—the dislike of one's body or insecurity about its attractiveness—is sometimes presumed to be a problem that disproportionately affects women.
The truth is, male fitness models and movie stars give men an equally distorted view of what an attractive male body is "supposed" to look like.
According to studies, 90% of all men and 95% of college-aged men express some dissatisfaction with their bodies.
The difference, according to Elliot Montgomery Sklar, is that "men are socialized not to discuss their body image concerns."
A study by Levitan, Quinn-Nilas, Milhausen, and Breuer discovered a strong correlation of poor body image with a range of male sexual dysfunction, including both erectile dysfunction and premature ejaculation.
Clinical depression affects 18% of all US men and correlates strongly with male sexual dysfunction.
Nobody knows exactly how depression relates to premature ejaculation. There is a "chicken-and-the-egg" dilemma at play here.
Sexual dysfunction may contribute to a patient's depression, but it has also shown to presage the premature ejaculation diagnosis as much as follow it.
Regardless, PE itself often has a strong neuropsychological component. An oversensitive penis isn't always the culprit.

A man's anxiety may not necessarily spring from past sexual experiences.
Generalized anxiety disorder also correlates with premature ejaculation. This type of anxiety can be caused by:
Men who worry or fret about their sexual performance may tend to suffer from a variety of sexual dysfunctions, including premature ejaculation.
Additionally, anxiety can cause men to fail to be present in the moment during sex.
This type of distraction can cause them to miss or misjudge the sensation that accompanies his ejaculatory "point of no return."
Several conditions can result in an overly sensitive penis, including:
Phimosis: a condition some uncircumcised men experience whereby the foreskin is so tight that it can't be pulled back from the head of the penis.
Trauma to the penis: resulting from injury or surgery.
High penile sensitivity is strongly correlated with a worsening of premature ejaculation according to a study published in the Journal of Nature.
Different parts of the penis could experience hypersensitivity. The effect on the ejaculatory response could be minimal, or it could be massive.
The foreskin is known to be particularly sensitive, leading some professionals to speculate as to whether circumcised men experience less sexual pleasure, less penile sensitivity, and (possibly) a lower occurrence of premature ejaculation.
However, the effect of circumcision on penile sensitivity, including as relates to premature ejaculation, is very inconclusive.
There is no evidence that circumcision strongly correlates with lower penile sensitivity and a lower likelihood of premature ejaculation.
Men have a particularly strong hormonal response to sexual intercourse with a new partner.
Some men are less able to control the ejaculatory response with a new partner than with a partner with whom they have established comfort and trust.
If the condition subsides on subsequent sexual encounters, there should be no cause for concern.
Remember, a precondition of premature ejaculation is that it causes the patient distress.
The distress of quick ejaculation may subside if the man and his new partner settle into a mutually satisfying sexual relationship.
The neurotransmitter serotonin may play a role in sexual arousal and appetite.
Men with primary, persistent premature ejaculation tend to exhibit less neurotransmitter activity in the area of the brain linked to the ejaculatory response.
This suggests a link between low serotonin activity and premature ejaculation.
Type-2 diabetes, a chronic progressive inability of the body to absorb glucose due to insulin deficiency, has a well-documented impact on sexual functions and can contribute to premature ejaculation.
When blood sugar levels get out of control, they can damage the autonomic nervous system, which plays a key role in blood flow, sexual arousal, and ejaculation.
This kind of damage is called diabetic neuropathy. Lack of ejaculatory control is a common side effect.
One of the most common forms of prostate disease is prostatitis, an inflammation of the prostate.
Pain from prostatitis can cause a number of sexual dysfunctions, including ejaculatory disturbance.
Treatment of prostate disease, including localized treatments of prostate cancer, has also been linked to sexual dysfunctions like premature ejaculation.
Alcohol and illegal drugs like cocaine have a reputation for causing erectile dysfunction.
However, they can also cause premature ejaculation.
Doctors recommend that patients suffering from premature ejaculation limit alcohol consumption to 2-3 drinks and avoid illegal drug use.
Substance-related illegal drug use can result in sexual dysfunctions that persist for years after the use of the substance is discontinued.
However, the effect mostly applies to:
Treatment of premature ejaculation usually involves some form of behavioral therapy.
A urologist may recommend a regimen of exercises designed to naturally increase time to ejaculation through practice, training, and muscle memory.
Note; Exercises may take a long time to master, so men and their doctors must keep an eye on morale.
Treatment plans may also include over-the-counter or prescription medications.
Below is a list of the most popular at-home and Rx treatment options for premature ejaculation.

The edging method is a behavioral method of learning ejaculatory control. It is easy for men to practice at home, either during masturbation or with a partner.
Tangible results may take time and dedication to achieve, so it is important to embark upon the treatment with patience and manageable expectations.
Berating yourself for not improving fast enough will not help.
The stop-start method works because it helps a man learn to identify the physical sensations associated with his "point of no return."
This is a euphemism for the level of physical arousal after which orgasm, and ejaculation are unavoidable.
This method allows a man to build knowledge of his "point of no return" into his muscle memory, so he can adjust the level of stimulation accordingly and avoid crossing it.
In this way, you can learn to delay ejaculation, more or less at will.

Click here to see our ultimate guide to master the edging method.
It bears repeating—the stop-start method takes practice.
Most men who suffer from premature ejaculation will sail right over the point of no return repeatedly before they learn to identify it. This is part of the process.
Without crossing it, you can't know what it feels like. The stop-start method is an occasion to focus on it and learn what it feels like.
The stop-start method also retrains the man and his penis on what to expect from sexual stimulation.
Most men follow a pattern of arousal whereby stimulation ramps up on a continuous upward incline, past the point of no return and then a rapid increase to climax, followed by a steep decline of arousal and relaxation.
For men with premature ejaculation, the ramp-up to the point of no return is particularly steep.
The stop-start method recreates the arousal curve.
There's still a steep ramp-up of arousal, but then the man uses repeated interruptions of stimulation to "hover" in a state of high arousal for an extended period of time, with slight increases and decreases in excitement but mostly a flat plateau.
When you decide you are ready, you can sustain stimulation past the point of no return and experience orgasm.
Over time, this plateau state of high sexual arousal may become ingrained in your muscle memory. You may learn to sustain it over an extended sexual session without ejaculating.
A variation on the stop-start method, the Squeeze Technique was pioneered by Masters and Johnson in the 1950s.
The technique, as the description might suggest, involves stopping sexual stimulation near the point of no return and squeezing the head of the penis, just below the frenulum (the ridge below the glans or head) to dull the ejaculatory response.
Note; that the goal is not to keep yourself from ejaculating after the point of no return.
Once you have achieved your orgasmic response, ejaculation is happening whether you let it out of your penis or not.
If anything, the semen might back-flow into the bladder and cause discomfort.
Instead, the point is to avoid the point of no return by decreasing the level of stimulation quickly, rather than waiting 30 seconds for it to subside naturally.
Squeezing the head of the penis rapidly decreases its level of arousal, allowing you to resume sexual activity more quickly.

Like the stop-and-start method, the squeeze technique can be practiced solo or with a partner.
The partner can even be the one who applies the squeeze. If you want to try having your partner apply the squeeze, make sure to practice beforehand with your erect penis, guiding the partner's hand and showing them where to squeeze and how much pressure to apply.
Aware of the sensitivity of the testicles, many women underestimate how much pressure the head of the penis can take without causing discomfort.
See our full guide on the squeeze technique for early ejaculation here.
One of the easiest medication-based treatments for premature ejaculation involves the use of a desensitizing spray like Promescent Delay Spray.
Available over the counter without a prescription, these sprays usually contain a topical anesthetic.
When properly formulated, the desensitizing spray can cause the penis sensations to become slightly muted.
In this state of desensitization, the penis may not experience such intense arousal from contact with the vagina or other sources of stimulation.
Without the steep arousal curve, a man may be able to achieve much greater performance in bed than he would without the medicating spray on his penis.
The two most common medications used in desensitizing sprays are:
It may be injected into the site of surgical incisions to relieve pain. It is also used in creams and oral anesthetics.
Things to look for in an effective desensitizing spray include:
A desensitizing spray can be applied 5-15 minutes before sexual activity and rubbed into the skin for even coating.
Experiment with the amount of medication you apply to discover the dose that gives you the best results.

Promescent® Delay Spray is a favorite among medical professionals and recommended by over 2000+ to help men last longer in bed.
Get a bottle of Promescent desensitizing spray today!
A certain component of premature ejaculation may be physical or hormonal. However, psychological factors may also contribute to early ejaculation, particularly:
A man may face particularly strong self-confidence issues if premature ejaculation has been a longstanding problem for him.
Fear of premature ejaculation may actually cause premature ejaculation to keep happening. Sex therapy may be an effective solution to treat the underlying psychological causes of PE.
Undertaken either individually or as a couple, sex therapy does not involve having sex in a therapist's office.
It's a cognitive approach to resolving psycho-sexual issues through communication and mindfulness.
A therapist will ask you and/or your partner probing questions relating to your sex life and your life in general. The therapist may then recommend strategies such as:
Therapy can make you conscious of the psychological roadblocks to delay ejaculation that may have been hiding deep within your conscious mind.
By becoming more mindful of them, you can start to implement strategies to counteract them.
Certain sexual positions are better for increasing the time it takes to reach climax. They do this by:
Examples of sex positions to try for increased IELT include:

With the woman on top and upright, she's in the "saddle" and in control of the session.
She can focus on her pleasure and strip the man of the temptation to seek his orgasm quickly.
Make sure the partner knows not to go too fast, or she could overstimulate you. Deep grinding with manual clitoral stimulation often works well for both partners.

The back-to-front spooning position limits the length of the strokes possible and may prove effective in stimulating the woman's "G-spot."
Note that the head of the penis is the most sensitive part of the organ. A man must monitor his point of no return, even with short strokes.

Lying on each other's sides and face to face, you and your partner can both control some of the thrust while giving up some of the control. The added effort to maintain this position acts as a distraction as well.

In this seated face-to-face position, a man's motion is restricted by the partner's body weight in his lap, preventing him from vigorous thrusting.
This position also limits the couple to short strokes and takes concentration to keep both bodies in position.
Instead of penetrating the vagina with the penis, consider rubbing it on the outside, stimulating the clitoris. One way to keep from becoming overly aroused by penetration is to skip the penetration!

In this position, the man lies on his side, the woman on her back, legs draped over the man's hips, genitals aligned for penetration.
A man's range of motion is very limited in this position, controlling the stimulation available to him.

Whereas Doggystyle usually results in deep penetration, laying both the woman and the man on their bellies, one on top of the other, greatly reduces the depth of penetration available to the man.

With the woman on top, she can take your penis inside her deeply without you having the range of motion to thrust, limiting the likelihood of overstimulation.

With the woman in control of the penetration depth, she is likely to let gravity do its thing and enjoy deep penetration without enough stroking to push you over the edge.

From missionary position, thrust deeply and stay in deep, grinding your pelvis against the woman's clitoris for added arousal. Without thrusting rapidly in and out, your penis may become aroused less quickly.

With the man standing and the woman lying on the edge of the bed, the man has ultimate control of how much stimulation he received.

In this position, the man kneels and lifts the woman's hips onto his lap and into alignment. The weight of the hips and the angle of the thighs limit the man's ability to thrust deeply.
You may find that different positions are more conducive to delay ejaculation. One man may find that more control of the thrust depth allows him to limit the amount of stimulation he receives in each thrust.
Another man may find this too big of a temptation to overstimulate; he may do better with a restricted range of motion.
If you want to learn more about these positions and how to do them, see our full guide here.
Dr. Arnold Kegel developed his signature routine of lower-pelvic muscle training as a treatment course for women with various forms of pelvic floor dysfunction.
The fact that Kegel's help women achieve fantastic orgasms was a pleasant bonus effect.
Less well-known is the fact that Kegel exercises can benefit men as well, particularly in the treatment of premature ejaculation.
One study noted an increase in IELT on 82.5% of male test subjects who practiced a routine of Kegel exercises.
Kegel exercises strengthen and tone the voluntary, skeletal muscles on the floor of the pelvis.
The anterior pelvic muscles can be flexed by squeezing as if you are trying to cut off the flow of urine to your urethra.
The posterior pelvic floor muscles can be flexed by squeezing your sphincter as if trying to prevent yourself from having a bowel movement.
Practice over the toilet if need be.
Strong Kegel muscles can not only help you delay ejaculation; they can help you have stronger orgasms, maintain stronger erections for longer periods of time, even experience multiple orgasms.
Kegel exercises are generally practiced two different ways:
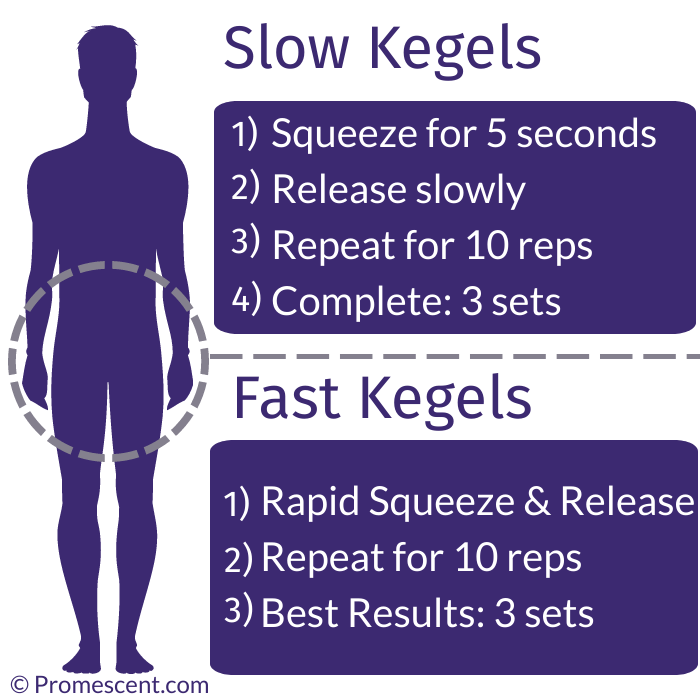
Squeeze your pelvic floor muscles and hold for a count of five seconds.
Remember to breathe.
It is tempting to hold your breath in a contracted Kegel position, but remind yourself to breathe normally.
Release and repeat ten times.
Squeeze the pelvic floor muscles and hold for a count of one second.
Release and repeat ten times.
Committed gym rats may be shocked to discover how much this invisible exercise, working out a relatively small muscle group, can wear you out.
Indeed, a full cycle of ten, slow, and ten fast Kegels may be more than you can endure as a beginner.
As with any gym routine, keep at it and gradually increase the load.
Strong pelvic floor muscles benefit a man's sexual health in a number of ways.
View our ultimate guide on how to successfully do Kegels to last longer in bed.
Condoms have a crucial role to play in safer sex practices, not only preventing unwanted pregnancy but also controlling or stopping the spread of certain sexually transmitted infections.
Some people don't like condom use during sex, claiming that it reduces the sensation and intimacy of the act.
This is debatable, but the tendency of some condoms to reduce the sensitivity of the penis can actually be a positive for men who struggle with premature ejaculation.
Any condom might accomplish the task of delaying the point of no return, although ultra-thin, "his pleasure" condoms may not be the way to go if the goal is to limit stimulation.
Some condoms, however, are specially designed for that task.
Delay condoms usually feature inner lubrication with benzocaine anesthetics. This numbs the penis, in addition to the desensitizing latex barrier.
Other condoms are designed with female pleasure in mind.
This might include lubrication, studs, or ribs. Lubrication may add to the man's stimulation—not good for increasing IELT.
However, if the vagina or anus is too dry, penetration might be uncomfortable for the partner.
Make sure to balance the needs of both partners when shopping for condoms.
When faced with long courses of treatment involving exercises and talk therapy, it is normal for a man to wonder why there isn't just a pill to reverse the condition.
After all, effective pills exist to treat erectile dysfunction.
Unfortunately, no perfect cure for premature ejaculation exists in modern pharmacology.
Certain prescription or even non-prescription medications may help certain men manage premature ejaculation.
While they enjoy limited acceptance in modern medicine, herbal remedies for various ailments have thousands of years of historical use to back them up.
Some over-the-counter herbal remedies make bold claims about their ability to increase stamina and make you last longer.
They vary wildly in ingredients. None of them come with a widespread stamp of approval from medical science.
No studies attest conclusively to their effectiveness.
If individual men find that they help, great. Most of the herbs are not toxic.
However, without FDA controls on their processing, you never really know what you are putting in your body.
Two studies, in 2005 and 2010, point to the possible effectiveness of St. John's Wort in treating premature ejaculation, but these studies are far from conclusive.
Still, it's common to see St. John's Wort in these remedies.
A certain type of antidepressant medication called Selective Serotonin Reuptake Inhibitors (SSRI) may be effective in treating premature ejaculation.
SSRIs allow serotonin to remain active in the brain for longer periods of time.
In addition to having a beneficial effect on the patient's mood, serotonin also plays a role in sexual arousal and ejaculatory response.
Serotonin deficiency is one of the suspected physiological causes of premature ejaculation.
Popular SSRIs include:
For all of these medications, however, treatment of premature ejaculation remains an "off-label" use, at least in the US.
They are FDA-approved drugs and a doctor can prescribe them for any reason (s)he sees fit, but the FDA has not approved the drug for this specific use—hence, "off-label."
One SSRI is approved to treat premature ejaculation, but it is not in the United States.


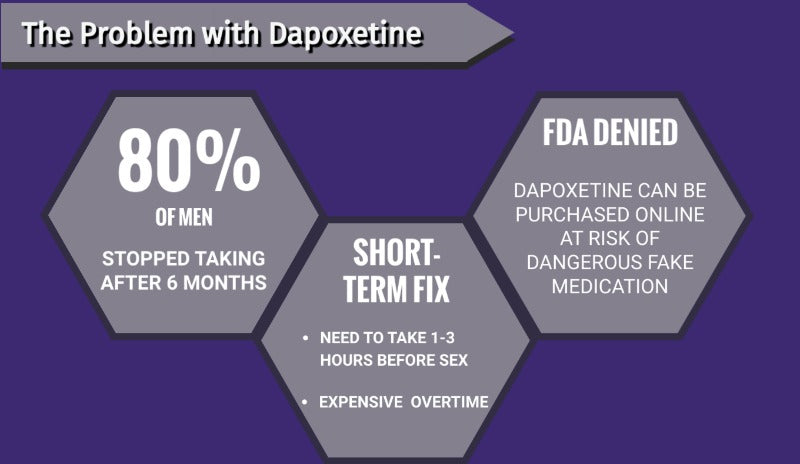

The SSRI Dapoxetine has a very short half-life, making it a less-attractive long-term treatment for depression.
However, in clinical trials, male users reported an increase in IELT of several minutes.
Despite these promising results, Dapoxetine was rejected as a treatment for premature ejaculation by the FDA in 2005 and has remained in Phase III of clinical trials ever since.
Other countries, however, have approved Dapoxetine for on-label use, including:
Dapoxetine has a high discontinuation rate in these countries, suggesting that men who use it are not satisfied with the result.
SSRIs are unpredictable in their effectiveness and known for having other side effects, including other sexual dysfunctions like ED and loss of libido.

Learn more about antidepressants (and their side effects) for premature ejaculation.
Viagra, Cialis, and Levitra are well known for their ability to reverse erectile dysfunction, producing rock-solid erections like magic.
Certain studies have shown that they also increase IELT, possibly by allowing the man to relax and enjoy sex, knowing that he doesn't have to worry about losing his erection.
For men who rush to orgasm because they fear losing their erections, this may make a big difference.
Levitra has demonstrated some of the best results in delaying climax.
Additionally, it may help men keep their erections after climax, allowing the sex session to continue for the benefit of the partner.
However, the studies on the effectiveness of ED medications in treating premature ejaculation are inconclusive.
Doctors generally recommend that men avoid taking erectile dysfunction medications unless they have ED or an indicator for a different off-label use.
Learn more about Levitra, Cialis, and Viagra for premature ejaculation.
According to a 2011 study published in the Journal of Sexual Medicine, women in relationships with men who have premature ejaculation reported more sexual problems.
They also reported reduced satisfaction, increased distress, and interpersonal difficulty, and issues with their own pleasure than those without.
The study found that premature ejaculation led both men and women to feel that “something is missing from the relationship and an impaired sense of intimacy.”
In a survey conducted by Promescent, 30% of married men who reported suffering from premature ejaculation reported feeling:
These feelings are consistent with wider scientific findings: a 2008 literature review in the Journal of Sexual Medicine concluded that premature ejaculation, “significantly negatively impacts men and their partners and may prevent single men from forming new partner relationships.”
Perhaps the scariest statistics came from a 2018 study, which found that 4.5 "bad sexual encounters" is the average number that spells the end of a relationship.

Consumption of alcohol often causes libido to increase. Inhibitions and anxieties drop, the brain enjoys a dopamine rush.
Heavy consumption of alcohol is associated with all sorts of sexual dysfunctions, especially erectile dysfunction (ED)—hence the term "whiskey dick."
Since it can dampen erections, it's natural that some men wonder whether they can turn "whiskey dick" to their advantage.
Since it gives some men difficulty in achieving orgasm at all, maybe it would delay the orgasmic response of an anxious or oversensitive penis.
This inference is not supported by medical science.
In fact, some evidence suggests that overconsumption of alcohol could cause premature ejaculation or make it even worse.
This might be due to the loss of impulse control that accompanies alcohol consumption.
If you want to correct premature ejaculation, getting drunk is the wrong way to go about it.
A vasectomy is a form of male sterilization.
The tubes that connect the testicles to the seminal vesicles (vas deferens) are severed surgically, permanently preventing sperm from entering the semen.
Vasectomy is a minimally invasive outpatient procedure, usually performed under local anesthetic.

When the swelling and pain subside in a matter of days, the patient can usually resume sexual activity as normal.
It may take several weeks and several ejaculations to purge the man's seminal tract of sperm that was already present in the seminal vesicle before the procedure.
As such, the patient should continue using other forms of birth control for at least three months after the procedure.
The tissues and mechanisms affected by vasectomy have no impact on arousal or the ejaculatory response.
A vasectomy will neither cause, nor reverse, premature ejaculation.
Learn more about how a vasectomy affects sexual performance.
A popular theory in the public consciousness claims that the removal of the sensitive foreskin from the penis causes reduced penile sensitivity in adulthood.
No conclusive studies point to any greater prevalence of premature ejaculation on the circumcised demographic of men vs. the uncircumcised demographic.
It doesn't seem to make any difference.
Circumcised men are just as likely to experience premature ejaculation as uncircumcised men.
After getting the bad news about the lack of a miracle pill, frustrated men in search of an aggressive and permanent treatment plan often inquire about the availability of a surgical cure for premature ejaculation.
Even an invasive surgery with a difficult recovery period may seem worth it, stacked up against a lifetime of disappointed sexual partners.
The news doesn't get any better.
All proposed surgeries to treat early ejaculation are in the experimental phase, the risks too high and the outcome too uncertain for any responsible doctor to recommend it.
Men are much better off using a delay spray or trying an exercise than they are putting their genitals under the knife.
Premature ejaculation does not correlate with low sperm count, infertility, or any other issues that might prevent a couple from conceiving a child.
The problem with PE isn't potency, it's that the sperm arrives too quickly, before either partner would welcome it.
That said, that speedy sperm is just as likely to be potent and capable of impregnating a woman.
If a couple cannot get pregnant, the male partner's premature ejaculation is most likely not the cause.
Some foods, like shellfish or pineapple, have purported aphrodisiac qualities or other sexual benefits. None of this is proven science.
However, what you put inside your body has a big impact on what you get out of it.
No food or diet is known to be an effective treatment for premature ejaculation.
If you want to eat right for your reproductive health, consider adding prostate-friendly foods like fruits, vegetables, and good fats, while eliminating libido-dampening goodies like sugar and red meat.
Learn about the top 10 foods that can help increase libido

A proper diet may also improve your sleep cycle and your mood, key components to healthy sexual functioning.
Drinking plenty of water also helps keep the urinary tract healthy and free from infection, as does eating antioxidant-rich fruits like blueberries and cranberries.
Testosterone plays a crucial role in a man's sexual health, regulating his libido, mood, and states of arousal.
Low testosterone can correlate with such symptoms as depression, loss of muscle mass, low sex drive, reduced appetite, and fatigue.
Low testosterone, however, does not correlate with cases of erectile dysfunction.
Studies into the testosterone levels of men suffering from premature ejaculation revealed statistically insignificant differences.
Acupuncture, an ancient form of therapy involving the insertion of thin needles into the skin at pressure points, has actually demonstrated promising results.
Studies comparing the effectiveness of acupuncture to treatment with SSRIs and a placebo revealed that acupuncture outperformed the placebo treatment but underperformed the SSRI.
The best results came from a blended treatment of acupuncture and an SSRI topical cream.
If you regularly have trouble delaying ejaculation longer than one or two minutes during sexual intercourse, consult your doctor.
While no miracle surgery or magic pill exists to cure it, premature ejaculation is a treatable condition that nearly one-third of all men will experience at some point.
Your doctor can recommend treatment plans and possibly refer you to a specialist.
When considering consulting a doctor about PE, ask yourself the following questions (and be ready to answer your doctor when (s)he asks them!)
The last two questions are not optional—in fact, they're two of the most important questions to answer.
Remember, the diagnosis of premature ejaculation requires that you feel distressed, shame, or other negative emotions as a result of your quick ejaculatory response.
In other words, your feelings do matter!
They are part of the medical diagnosis. If you think your performance isn't what it should be, speak to your doctor.
Premature ejaculation is the most common sexual dysfunction a man can expect to face.
Between 20-40% of all men will cope with it at some point in their lives.


Most of the time, many of these factors contribute to a diagnosis.
Almost every man wants to be a great lover, capable of satisfying his partner on a regular basis.
The inability to do so may make you feel like a failure as a man.
People can believe what they want about the relative masculinity of different IELTs, but the fact remains that premature ejaculation can be treated.
Delaying ejaculation may not be an easy goal to achieve, but worthwhile goals rarely are. The only way you could really fail is to not even try.
Once you commit to treatment, several avenues open up to push back against premature ejaculation, including:
Different men cope with premature ejaculation in different ways.
Some are resolute, some depressed. Some get frantic and anxious, others apathetic.
Some doubt that they will ever get better, feeling like they're doomed to have an unsatisfying sex life.
The truth is, the sex life of a man who copes with premature ejaculation is very much in his own hands. And no, that's not just a masturbation joke.
Many men (and women) cope with much greater challenges and go on to have rich, fulfilling lives—including satisfying sex, relationships, and parenthood.
With a proactive approach, men can beat premature ejaculation.
Absorption Pharmaceuticals LLC (Promescent) has strict informational citing guidelines and relies on peer-reviewed studies, academic or research institutions, medical associations, and medical experts. We attempt to use primary sources and refrain from using tertiary references and only citing trustworthy sources. Each article is reviewed, written, and updated by Medical Professionals or authoritative Experts in a specific, related field of practice. You can find out more about how we ensure our content is accurate and current by reading our editorial policy.

reviews
Your Cart Is Empty














